MERCURI-3 — should patients already on an SGLT2 inhibitor keep taking it through cardiac surgery?
A multicentre, randomised, open-label superiority trial testing whether continuing an SGLT2 inhibitor through cardiac surgery protects the kidney better than the interruption recommended by current guidelines.
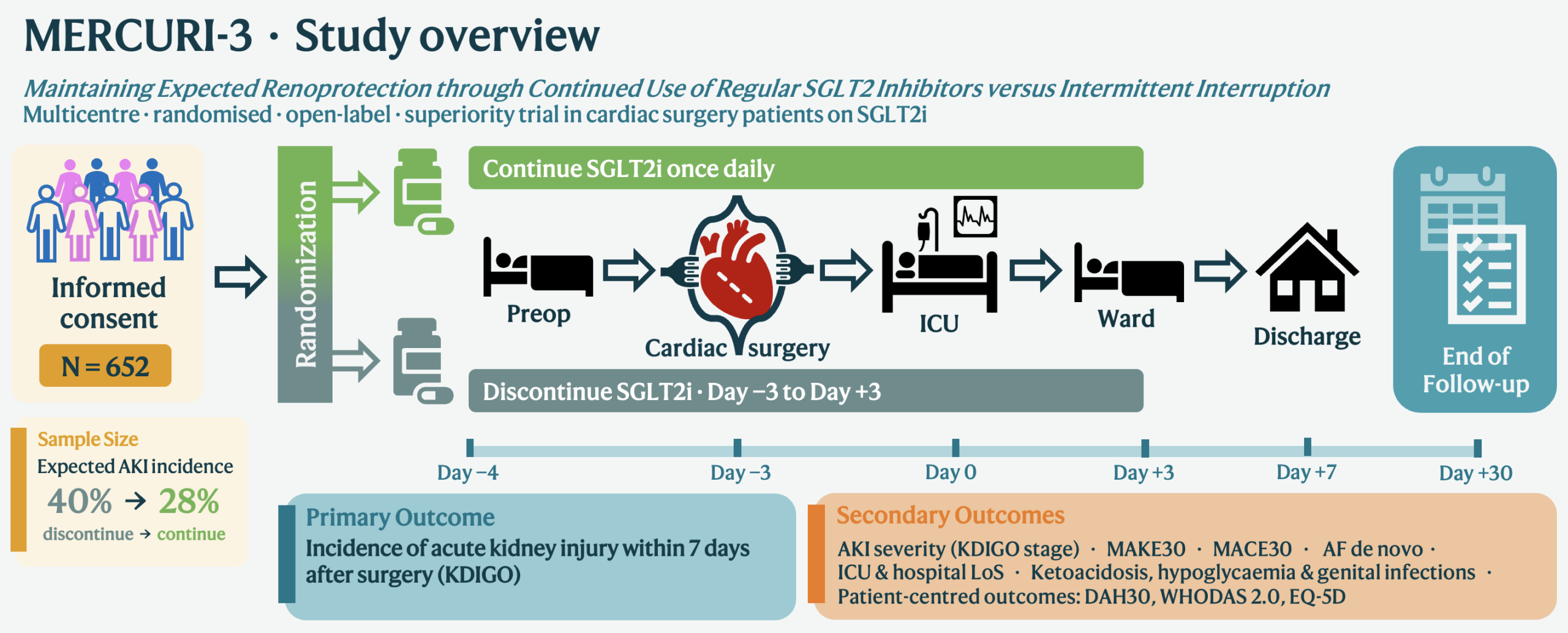
MERCURI-3 stands for Maintaining Expected Renoprotection through Continued Use of Regular SGLT2 Inhibitors versus Intermittent Interruption. Funded by ZonMw (Goed Gebruik Geneesmiddelen) under the grant title SIRIUS — SGLT2 Inhibition Rules In patients Undergoing Surgery — project 10141022510066. Trial registration details will be added here once available.
The problem
SGLT2 inhibitors are increasingly prescribed to patients undergoing cardiac surgery, many of whom already take one for heart failure, chronic kidney disease or diabetes before they ever reach the operating table. Current guidelines advise stopping these drugs several days before surgery, a precaution based on early concerns about perioperative ketoacidosis, at a time when the risks and benefits of continuation were poorly understood. Our group’s earlier MERCURI-1 pilot trial found that starting an SGLT2 inhibitor perioperatively in previously untreated patients lowered the incidence of acute kidney injury (AKI) from 67% to 20% (published in Journal of Clinical Anesthesia, 2025), and the confirmatory MERCURI-2 trial has completed follow-up, with its manuscript in preparation.
MERCURI-3 asks a different question. Rather than whether to start an SGLT2 inhibitor before surgery, it asks whether patients who are already taking one chronically should keep taking it through the perioperative period, instead of interrupting it as current guidelines recommend. Outpatient trials in diabetes, heart failure and chronic kidney disease consistently show SGLT2 inhibitors protect the kidney, and reports of perioperative ketoacidosis have been rare in more recent surgical cohorts. Interrupting a chronic medication also carries its own risks, including rebound heart failure, and a pragmatic, low-burden answer is needed for the many patients who now arrive for cardiac surgery already on these drugs.
Design
A multicentre (academic and non-academic), international (the Netherlands and Belgium), randomised, open-label superiority trial. Patients already treated with an SGLT2 inhibitor are randomised at least 4 days before cardiac surgery, using minimization to balance groups by centre, sex, diabetes status and indication for SGLT2i use. The continuation arm keeps taking their SGLT2 inhibitor once daily before, on the day of, and after surgery; patients with diabetes also receive a perioperative glucose–insulin infusion to mitigate ketoacidosis risk. The discontinuation arm follows current guidelines, stopping the drug three days before surgery until three days after (seven days in total). Blood ketone concentrations are checked in all participants before surgery and one hour afterwards as an additional safety measure.
The primary outcome is the incidence of acute kidney injury according to KDIGO criteria within the first seven days after surgery. Follow-up has been extended to 6 months to allow evaluation of kidney function, major adverse cardiovascular and kidney events, patient-reported outcomes (WHODAS 2.0, EQ-5D-5L, DAH-30) and the health-economic evaluation (cost-effectiveness and cost-utility analysis) over a longer horizon than the perioperative period alone. Following referee review, the sample size was increased to 652 patients (326 per arm), powered at 90% to detect a difference between an assumed AKI incidence of 40% in the discontinuation group and 28% in the continuation group.
Status
The grant was awarded in July 2026, following referee review and a rebuttal in which the study design was refined (sample size increased, follow-up extended to 6 months, minimization added to the randomisation strategy). The project is in its start-up phase: ethics submissions (METC), data management planning and site agreements are being finalised across the Netherlands and Belgium. Recruitment is expected to begin in 2027, with an inclusion period of roughly 24 months across the seven participating centres.
Participating centres
Amsterdam UMC
Amsterdam, the Netherlands (coordinating centre)
UMC Groningen
Groningen, the Netherlands
Amphia
Breda, the Netherlands
Medisch Spectrum Twente
Enschede, the Netherlands
Medisch Centrum Leeuwarden
Leeuwarden, the Netherlands
UZ Leuven
Leuven, Belgium
ZOL Genk
Genk, Belgium
A Trial Steering Committee oversees design, execution and completion, with two Belgian members responsible for trial conduct at UZ Leuven and ZOL Genk. Day-to-day coordination is led by the PhD candidate, supported by a research nurse at each site.
Team & collaborators
Alongside the site investigators above, the project team includes Jimmy Schenk (statistics/epidemiology), Annelies Visser (implementation), Veerle Coupé (health-economic evaluation), Goos Laverman (nephrology), Susanne Eberl (cardiac anaesthesia), Marcella Müller (intensive care), Tomas Cherpanath (intensive care/cardiology), Nimrat Grewal (cardiothoracic surgery) and Hans van Goudoever (administrative lead, Amsterdam UMC). Professional societies embedded in the project team include the Dutch Association of Anaesthesiology (NVA), the Dutch Society for Thoracic Surgery (NVT), the Dutch Internists Association (NIV), the Netherlands Society of Cardiology (NVVC) and the Dutch Federation of Nephrology (NFN).
Associated organisations
ZonMw


Where this leads
MERCURI-3 is the next study in the MERCURI line: MERCURI-1 and MERCURI-2 asked whether to start an SGLT2 inhibitor before cardiac surgery; MERCURI-3 asks whether patients already taking one should keep taking it. Its ZonMw GGG grant, SIRIUS, sits alongside the separate GGG grants that fund GUIDE and MERCURI-2.